Medication - Blog Posts
I saw a post saying that stimulants for ADHD are life saving medications because they reduce car crashes and while stimulants are very important for people with ADHD they just... aren't life saving.
some medications you will die without. stimulants for ADHD are not on that list.
when other disabled people talk about life saving medication we don't just mean "very important" we mean "life saving"
I would die of organ failure caused by inflammation from lupus if I didn't have my biologic. diabetics would die of diabetic ketoacidosis without insulin. people with asthma would suffocate to death without their inhalers. that is what it means to have a life saving medication.
you can emphasize the importance of a medication without comparing it to truly life saving medications. it just comes across really insensitive when you compare lower risk of car crashes to guaranteed death without a medication
like, the shortage of stimulants is absolutely detrimental to people with ADHD but it's not comparable to a shortage of a life saving medication. without a stimulant people with ADHD would still live, without insulin diabetics would die. when stimulant prices are inflated and people can't access them it is hard but it does not equate to death. when people with life threatening autoimmune diseases can't afford their medication it does equate to death.
if you want to talk about the importance of stimulants for people with ADHD and the negative effects of the shortage that's great! but refer to the medication correctly- it's life changing, it's not life saving


That would help so much

Doodle dump/sloppy half-rendered comic page. I’ll arrange it in a more readable order eventually. Story info under the cut.
Noryn broke his ankle during a mission and then ran on it for a while before the adrenaline wore off and he really noticed what happened. The healers are preoccupied with people more fucked up than he is, but luckily his bodyguard is trained in enough first-aid/healing to set it and help him get comfortable-ish until someone can fix it properly.
He has an anxious aversion to drugs/pain medication after some unsavory experiences in his younger days and getting him to take anything can tend do be a bit of a fight, but Rük is always a calm voice of reason, even when he’s screaming inside.

Dudes healthcare is so fake. My ADHD meds are $940 without insurance. But they gave me a website of "coupons" which straight up looks like a scam website, and I got it today for $60! Just a coupon from a random website and it was $900 cheaper. America, I am confusion!! America explain!!
Today, all I have is medication and lemonade, and I forgot to take my meds.

I ran out of meds and I'm now feeling the symptoms of abstinence. Going to collect more.
Wish me luck.

finally getting the medications which will help me with my forgetfulness is amazing
i hope i don't take the med i'm suppose to take on a specific day today, aka not the specific day
i woouldn't really
haha
Long post time!
I once was on a medication that worked rather well for what I needed but unfortunately gave me unusual vivid dreams every night. For your amusement (and because this vent is long-awaited), I am compiling a list of the types of dreams I had and their ratings!:
Dreams where I drive: 4/10. Not the usual car crash dreams, which tbh are about a 6/10 because they're kind of terror-inducing in a rollercoaster way. These driving dreams, however, are normal driving stints, which means I often forget in my waking hours which memory of parking the car was the actual place I parked my car and which ones were dreams. >:(
Dreams with my significant other: 6.5/10. Easy to tell they're not real, yet still enjoyable, and usually involving other people s/o hasn't interacted with, so I get to see some new character interactions.
Dreams that are wholly focused on dream!me trying and failing to fall asleep: 2.5/10. Those suck. It kind of just makes my waking hours of falling asleep even worse, and leaves me pretty frustrated the next day.
Dreams where I am inexplicably in random, mundane places: 3.5/10. The problem with these is that they're fairly unsettling, and they stay with me a while, leading to some weird deja vu of "I've been here" when it was in fact a very clear dream I had weeks ago.
Dreams that splice in weird bits of trauma: 1/10. Shut up. This literally isn't relevant anymore and you have no reason to be bringing this up and dragging other innocent parties (random people in my dreams) into this.
Dreams that take a week or longer in a single night: 5/10. You get trapped in there and watch days pass, but usually if I'm having one of those dreams the location ain't bad. Brain has to sustain something for a week, after all. It very often gets overwhelming toward the end of the week, which might push it to a lower rating, but the locations generally being optimistic push it up a rating, so it balances out. The curse here is that I remember a week that never happened.
Dreams that are educational: 5.5/10. Pretty random, but not usually haunting, so that's a bonus. I could probably write an encyclopedia of absolute gibberish from the things I've learned from my dreams. They make sense, in a weird way, but some of the diagrams feel AI-generated? Even though it's in my head? And some of the concepts, too. Legit I have read textbook chapters in my head of knowledge that either I didn't know or isn't real, or both. (Usually the latter.)
Dreams that just tell me stuff that happened recently in real life: 4/10. There's almost always a negative tint and it's like, bro, why are you telling me this, I was there, I lived it this afternoon. And then my concept of what actually happened is messed up the following days, weeks, whatever.
I might come back to this and update it if I remember more types of dreams I've had. Or if I look in my notes app tbh. But anyway, having vivid dreams every night that haunt your waking life are not normal, so if you were wondering about yourself, you might want to check on that with a medical person, especially if it's impacting your memory or how rested you are each day. I had a long time being hesitant/resistant to call them "nightmares," because most of the time it wasn't scary monster or hopeless scenarios where I end up dying or worse, but the definition of nightmares isn't as rigid and black-and-white as we thought as kids. Bad dreams? Unsettling dreams? Dreams that bother you at all? Those are nightmares. It's not childish, and it is not something you need to live with.
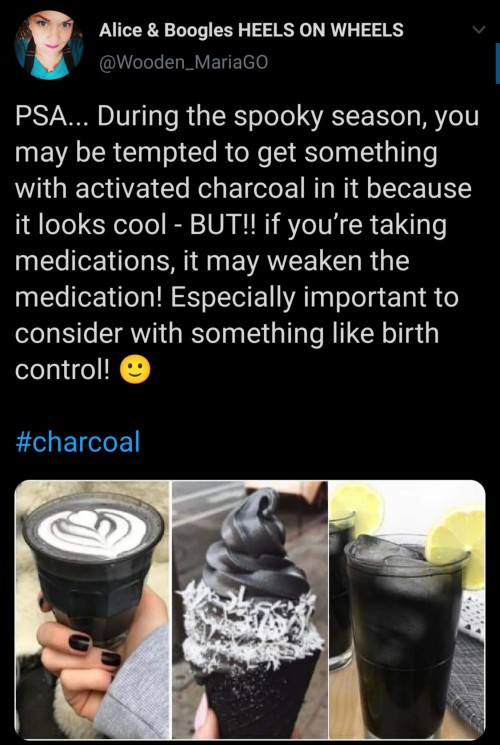
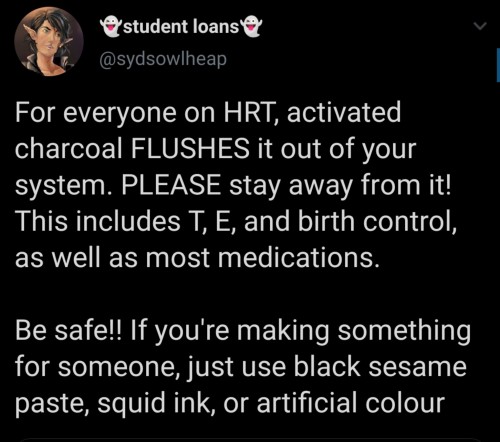
Reposting for peopel like me who are on one or more of these and didn’t know this

Just a little PSA for all our mental health (and chronic pain*) spoonies out there! A lot of doctors neglect to mention this little side effect, which means a lot of us are suffering extra from the heat without knowing why.
*Many psych meds are used to treat chronic pain as well, if you didn’t know!
I just realized that all my medication sounds like Pokémon names. Like "I choose you, Lexapro!" or "My eevee evolved into a Bupropion."
You know the medication is working when it has you looking up bipolar disorder
Common ototoxic medications
"FAV Q&A"
Furosemide (and other loop diuretics) Aminoglycosides Vancomycin Quinine Aspirin
Not being able to afford your drugs is a hell of a drug.
Don't know what I'm supposed to feel on these meds... Is depression medication supposed to make you feel happy? That's not the case right now, for sure. Maybe just slightly less miserable? And a little less clouded over? Maybe there's no medication to fix what I am.
Not gonna get into it but having medical problems and getting very unlucky dude I had to crawl my way downstairs partially deaf and unable to move my eyes in their sockets (cuz pain scale 9 yeouch) (had to close my eyes every time I moved and only open them when I’m perfectly still like some kind of horror game) and like it was pretty freaking surreal having like no sleep feeling my way down the stairs in the house at 5:36 am lmao.
Felt kinda liminal, or maybe it was the migraine making me stupid idk 💀
But I was low-key feeling like an ego death or smt I felt like a creature on this planet bro.
Still don’t have my hearing back but hopefully it comes back eventually???? Cuz I can’t take the meds to fix it because it will react with my heart medication😔
Anyways I love pain meds <3
My fav part of antidepressants is that I’ll wake and up and wonder “why should I get out of bed?” And not find and answer, but then be like “I don’t need a reason ima get up cuz I want to” :D
Not your boomer family getting mad at you for messing up your medication's concentration and hurting yourself ONCE as if they didn't drink margaritas for pregnancy pain and smoked cigarettes against asthma.
My meds have been adjusted, and this is day three on the new dose. I am not doing well. We don't know if my body is metabolizing them, so this is doubling the dose to see if it takes. I am dissociating and I feel stuck in a dream. I don't know what to do with myself. I just want to cry.
My cheque I've been waiting a few months for and was supposedly delivered one week ago is now beyond a doubt either stolen or missing. (:
Let’s end the stigma of shame around taking medication for mental illness.
When you take medication, it means you are intelligently using the resources available to you, so you can live the best life possible. This is a beautiful and self-loving action.
Okay and encouraged to reblog if you live with or without mental illness.
I fully recognize that this probably won't get much attention, but a friend of mine needs help, and I can only do so much. Did manage to talk them into starting a GoFundMe, but I know for a FACT that they didn't list all the problems they're having. If you can help them out, I'd be grateful.


Demon Of Pain - Day 1

Going thru withdrawal again. Day 1 without seroquel (a sedative). Wish my sanity luck cause my insomnia came back with a vengeance.
Drew this when I got off of effexor almost a year ago.
My fibromyalgia is a bitch to deal with when it comes to withdrawal. Last time I was often bed bound for a month and then after gradually got my strength back while dealing with less withdrawal symptoms, and at the time I felt like I had lost my sanity. That my mind had fractured from the pain.
It's taken months and therapy to get where I am now. I'm stronger for it. I know I can make it through this, and I know what to do when I get overwhelmed now.
Still. Not looking forward to the upcoming breakdowns.
I'll most likely be posting a lot to the void on this account during this time btw, cause thats what I did last time (on a different site that my family follows so fuck that this time around). It helps for some reason.
Welcome to the Demon of Pain series where you'll be following this demon in its natural habitat... pain 😌
i might be put on antipsychotics… :(

Pneumonia In Children And Adults

Introduction
Pneumonia stands as a prevalent respiratory infection, exerting a significant burden on global public health. Its impact extends beyond mere morbidity, contributing to substantial healthcare costs and socioeconomic consequences. This discussion aims to elucidate the general nature of pneumonia, encompassing its pathophysiology, clinical presentation, diagnostic modalities, treatment strategies, complications, and preventive measures. By indulging into these factors, we aim to provide a better understanding of pneumonia’s complexity and underscore the importance of timely recognition and management.
Pathophysiology

Pneumonia ensues from the infiltration of infectious agents, including bacteria, viruses, fungi, and less commonly, parasites, into the lower respiratory tract. Upon inhalation or aspiration of these pathogens, they gain access to the alveoli, where they incite an inflammatory response. This inflammatory cascade triggers the release of pro-inflammatory cytokines and chemokines, recruiting immune cells to the site of infection. Neutrophils, macrophages, and lymphocytes converge to eradicate the invading pathogens, leading to the characteristic consolidation and exudate formation within the affected lung tissue. As the infection progresses, alveolar edema, impaired gas exchange, and parenchymal damage ensue, culminating in the clinical manifestations of pneumonia.
Clinical Presentation

The clinical presentation of pneumonia encompasses a spectrum of symptoms, ranging from mild respiratory complaints to life-threatening respiratory failure. Common symptoms include cough, productive sputum production, fever, chills, pleuritic chest pain, dyspnea, tachypnea, and systemic manifestations such as malaise and fatigue. The severity of symptoms varies depending on factors such as the underlying pathogen, the extent of lung involvement, the host’s immune status, and comorbidities. In pediatric populations, pneumonia may present with nonspecific symptoms such as feeding difficulties, lethargy, and irritability, posing diagnostic challenges. Conversely, elderly individuals may exhibit atypical presentations characterized by confusion, hypothermia, and exacerbations of underlying chronic conditions.
Diagnostic Modalities

The diagnosis of pneumonia hinges on a comprehensive clinical assessment, augmented by various diagnostic modalities to confirm the presence of pulmonary infection and reveal its etiology. A thorough history and physical examination provide invaluable insights into the patient’s symptomatology, risk factors, and clinical trajectory. Symptomatic findings such as crackles, wheezes, and diminished breath sounds may aid in localizing the site of infection and assessing disease severity. Radiographic imaging, notably chest X-rays and computed tomography (CT) scans, serves as the cornerstone of pneumonia diagnosis, revealing characteristic radiographic findings such as airspace opacities, lobar consolidation, and interstitial infiltrates. Laboratory investigations, including complete blood count (CBC), C-reactive protein (CRP), and procalcitonin levels, may corroborate the clinical suspicion of pneumonia and guide therapeutic decisions. Additionally, microbiological testing of respiratory specimens through techniques such as sputum culture, blood cultures, and polymerase chain reaction (PCR) assays facilitates pathogen identification and antimicrobial susceptibility testing, thereby informing targeted therapy.
Treatment Strategies

The management of pneumonia hinges on prompt initiation of empiric antimicrobial therapy tailored to the likely causative pathogen(s) and disease severity. Antibiotics represent the mainstay of treatment for bacterial pneumonia, with the choice of agent dictated by factors such as local antimicrobial resistance patterns, patient age, comorbidities, and recent antibiotic exposure. Commonly prescribed antibiotics include beta-lactam agents (e.g., penicillins, cephalosporins), macrolides, fluoroquinolones, and combination regimens for severe or healthcare-associated infections. Conversely, viral pneumonia necessitates supportive care measures, given the limited efficacy of antiviral agents in most cases. Influenza-associated pneumonia may benefit from neuraminidase inhibitors such as oseltamivir, while respiratory syncytial virus (RSV) pneumonia may warrant ribavirin therapy in select cases. Adjunctive therapies such as oxygen supplementation, bronchodilators, and corticosteroids may mitigate respiratory distress and improve clinical outcomes, particularly in severe or hypoxemic patients. The duration of antimicrobial therapy varies depending on factors such as the causative pathogen, clinical response, radiographic resolution, and the presence of complications. Close monitoring of clinical parameters and serial imaging studies guide the decision-making process, enabling clinicians to tailor therapy to individual patient needs.
Complications

Pneumonia harbors the potential for various complications, ranging from mild to life-threatening sequelae, necessitating vigilant monitoring and timely intervention. Common complications include pleural effusion, empyema, lung abscess, respiratory failure, septic shock, and acute respiratory distress syndrome (ARDS). Pleural effusion denotes the accumulation of fluid within the pleural space, secondary to inflammation or impaired lymphatic drainage, manifesting as dyspnea, pleuritic chest pain, and dullness to percussion on physical examination. Empyema represents a purulent collection within the pleural cavity, often complicating bacterial pneumonia and necessitating drainage via thoracentesis or chest tube placement. Lung abscesses manifest as circumscribed cavities containing necrotic debris and pus within the lung parenchyma, triggered by persistent fever, productive cough, and hemoptysis. Respiratory failure ensues from impaired gas exchange and alveolar hypoventilation, caused by worsening hypoxemia, hypercapnia, and respiratory acidosis, necessitating mechanical ventilation and intensive care support. Septic shock represents a life-threatening complication of severe pneumonia, characterized by systemic inflammatory response syndrome (SIRS) and end-organ dysfunction, requiring aggressive fluid resuscitation, vasopressor therapy, and broad-spectrum antibiotics. ARDS denotes a severe form of acute lung injury, characterized by diffuse alveolar damage, refractory hypoxemia, and bilateral infiltrates on chest imaging, necessitating lung-protective ventilation and supportive care in the intensive care unit (ICU). The occurrence of complications portends a poor prognosis and underscores the need for early recognition and intervention to mitigate adverse outcomes.
Preventive Measures

Preventing pneumonia entails a broad approach encompassing vaccination, infection control measures, and health promotion strategies aimed at reducing the risk of respiratory infections and their sequelae. Vaccination stands as a cornerstone of pneumonia prevention, targeting common bacterial and viral pathogens implicated in pneumonia pathogenesis. Vaccines such as the pneumococcal conjugate vaccine (PCV13) and pneumococcal polysaccharide vaccine (PPSV23) confer protection against Streptococcus pneumoniae, the leading bacterial cause of pneumonia, particularly in high-risk populations such as young children, older adults, and immunocompromised individuals. Influenza vaccination remains paramount in mitigating influenza-associated pneumonia and reducing disease transmission, underscoring the importance of annual vaccination campaigns targeting vulnerable populations. Additionally, adherence to infection control measures, including hand hygiene, respiratory etiquette, and environmental sanitation, plays a pivotal role in reducing the spread of respiratory pathogens in healthcare settings and the community at large. Health promotion efforts aimed at smoking cessation, optimizing nutrition, and addressing underlying comorbidities such as chronic obstructive pulmonary disease (COPD), asthma, and immunodeficiency bolster immune resilience and mitigate pneumonia risk. Furthermore, early identification and management of predisposing factors such as malnutrition, homelessness, and overcrowded living conditions attenuate pneumonia susceptibility and enhance overall health outcomes.
Conclusion
In conclusion, pneumonia emerges as a formidable respiratory infection, posing significant challenges to global public health. Its diverse etiology, clinical manifestations, diagnostic modalities, treatment modalities, complications, and preventive measures underscore the nature of pneumonia management. Timely recognition and intervention are imperative in mitigating the morbidity and mortality associated with pneumonia, necessitating a collaborative approach among healthcare providers, public health authorities, and policymakers. By fostering a comprehensive understanding of pneumonia’s manifest and implementing evidence-based strategies, we can strive towards reducing its burden and improving patient outcomes. Through ongoing research, education, and advocacy efforts, we can envision a future where pneumonia-related morbidity and mortality are substantially diminished, paving the way for enhanced respiratory health and well-being worldwide.
In managing pneumonia, compassion, empathy, and a holistic approach are essential alongside clinical expertise. Striving for excellence in knowledge and practice allows us to enhance respiratory medicine and patient outcomes.
As we address pneumonia and broader cardiovascular health complexities, let’s remain committed to optimal patient care. Together, we can impact lives positively and foster a healthier future.
Medical students encounter significant academic challenges during their studies, balancing coursework, clinical rotations, research, and personal commitments. Expert Academic Assignment Help offers tailored assistance to meet their needs, providing study materials, tutoring, assignment help, and exam preparation. Beyond academics, it fosters a supportive environment for mentorship and guidance. In essence, Expert Academic Assignment Help is a valuable resource for medical students, empowering them to excel academically and develop into competent healthcare professionals. Contact us at expertassignment46@gmail.com for professional assistance