Oncology - Blog Posts
REBLOG THIS. Doesn’t matter if it fits your accounts aesthetic, DO IT.
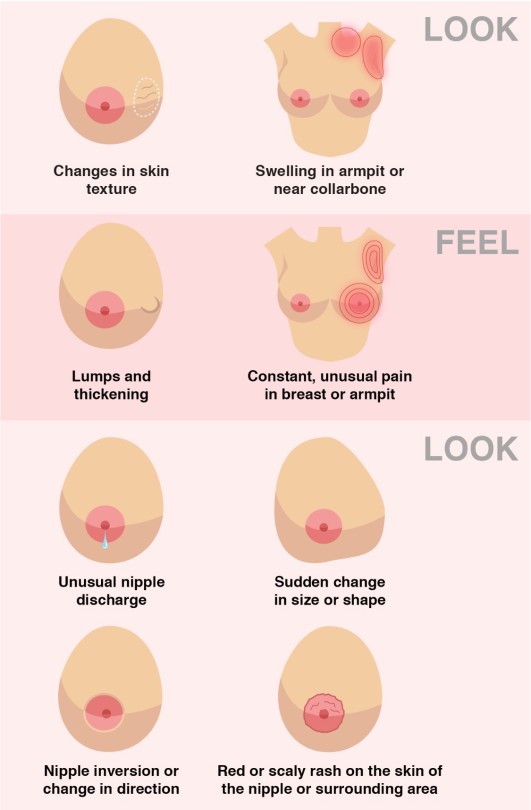
How to spot signs and symptoms of Breast Cancer
"RSV" g. house/j. wilson Oneshot
---------------->
The cold atmosphere surrounding the two men dampened the mood plenty, and the harsh coughs of the patient in front of them made it worse.
House had taken a case of a seven year old girl who hadn’t been able to walk since she was three. Whenever pressure was put on her left leg she would get a shooting pain all the way up to her spine.
No doctor knew why, other than that it was immovable and that she would probably never use it again. She and her mom had come into the clinic due to a respiratory infection, and House found her background ‘interesting.’
After a plethora of examinations and not-so-legal operations, he and his team found a tumor in her calf and in the middle of her spinal cord. How all of her other doctors missed them baffled the man, truly.
But that was how he was now sitting next to the girl showing her magic tricks as Wilson discussed with her mom possible treatments.
“We could remove them and the dead tissue that surrounds the tumors, but it’s a tough and long operation that doesn’t have the highest chance of working.” Wilson stated lowly to the crying woman.
“How high?” She choked out, wiping her eyes with a tissue.
“A good, twenty-percent chance.” He estimated and thought about the severity of the girl's illness. “Her respiratory infection also doesn’t help much in the process, but if we don’t take those tumors out now, they might not be able to come out at all.”
The mother looked over at her daughter and watched as House pulled out a card from behind her ear, and then she saw him flick the girl’s forehead when she said it was the wrong card. Her mother laughed slightly, and then looked back at Wilson.
“Where do I sign?” Wilson smiled at her words and nodded to the door, “I’ll show you the reception.”
=======
The woman came back to the room and hugged her daughter, kissing her forehead. “Are you ready to get better, sweetie?”
The girl nodded her head and grinned, a tear falling from her eye.
Wilson walked in and snorted at House, who had fallen asleep in the chair with cards spread out all over him.
“House.” He called out to the man, repeating it louder again. House still didn’t wake up, and Wilson scoffed before looking at the girl and the woman.
“It’s about to get a little loud.” He warned them before he stood in front of the girl and offered his hand out. She took it, and he used his other to take off a cord that connected her to her heart monitor. It beeped loudly, repetitively, and House jolted awake.
“Huh?”
“Welcome back, we almost lost you there.” Wilson said sarcastically, and House rolled his eyes. Wilson looked back at the girl, and he and House both grimaced when she coughed on his face.
“I am so sorry.” The girl said and covered her mouth as she finished coughing.
Wilson smiled tightly at her and connected her back to the heart monitor, “It’s all right, it happens more than you think.”
=======
“Where’s Wilson?” House barged into Cuddy’s office, completely ignoring the man she was with.
“House!” She scolded him, gesturing to the other man. “I’m in a meeting with someone. Knock next time.”
“Oh, really? In that shirt I thought you were trying to proposition him a little something-something, if you catch my drift.” He raised his eyebrows to punctuate his sentence and grinned.
Cuddy gritted her teeth, and excused herself from the other man before walking out of the office with House trailing behind her.
“Wilson is at home sick with RSV. I told him to leave when I saw him this morning with eyebags heavier than yours and when I heard him cough his lungs out in his office from outside his door.”
House looked at her and hummed before taking off without a word. The woman groaned and turned around, stopping one of the assistants. “Clock Dr. House out of work, please.”
=========
House lifted his cane up to Wilson’s door and knocked to the tune of ‘Shave and a Haircut’. He didn’t get a response, so he jiggled the handle and opened the door when he noticed it was unlocked.
“You know, I could kill and rob you right now.” He shouted out as he walked into Wilson’s living room. It was eerily quiet, and he didn’t like it. The man thudded his cane on the ground three times and heard a faint cough as three other knocks followed from Wilson’s bedroom wall.
House’s eyebrows furrowed and he went to see the sick oncologist, roughly opening the door and turning on the lights. “Wakey wakey, eggs and bakey.”
Wilson groaned loudly and grabbed one of his pillows to cover his head with, coughing underneath it. He groaned even louder when House poked him with his cane, right before House jabbed it into his side.
“Ow! House!” Wilson uncovered his head and looked at the other man, holding up his hand to the light above them. He coughed a bit, and House let out a quick ‘yikes’ when he saw just how bad Wilson looked.
The man in question had eyebags darker than his own hair, and his eyes were incredibly red and puffy. His lips were dry and cracked, and he had dried drool on his chin. His cheeks were red as well, and his hair was tousled like he just got thrown off a bull.
“Jesus Christ.” House murmured, taking in the sight of his best friend. The said man had only grunted and thrown his face back into his pillow, coughing into it.
“If you’re gonna gawk, at least turn the lights off.” His voice was muffled, but House understood it enough to flick the light switch and leave the room.
The man stood there for a second, staring at the door before going into the kitchen and grabbing Wilson’s keys from the glass bowl, and leaving to go to his own house.
=======
Wilson’s eyes opened when he heard his front door slam shut, and he inhaled deeply and sat up. He ran his hands through his tangled hair and carefully stood up, making his way to his bathroom. Washing his hands when he was finished with his business, he turned off the water and dried his hands while trying to sniff the air.
He couldn’t smell or breathe very well, but there was a slight smell of Thai food that caught his attention. He fixed his hair and left the bathroom, and wobbled to his kitchen, where he saw House sitting down on his sofa and eating noodles while watching ‘General Hospital.’
“Save any for me?” He croaked out and cleared his throat.
“Fridge.” Was the only thing House said through a mouthful of noodles, and Wilson made his way to his fridge.
He pulled out a box of more noodles, and noticed the grocery bag on his counter. He reached out for it, and pulled out a bottle of Nyquill, Aspirin, Tylenol, allergy medications, and Motrin.
He opened the bottle of Tylenol and grabbed two, tossing them into his mouth and fitting his head under the sink to down them with the tap water. He grabbed the Thai noodles and sat down next to House, digging into his food.
They both sat there in enjoyable silence until Wilson noticed all of the new pillows and blankets that sat on his reclinable sofa and spoke up.
“What’s all that for?” He mumbled through his noodles.
“Doesn’t matter.” House said simply, pushing himself off the couch with his cane and taking his trash and bowl to the kitchen. Wilson stared at the cushions and shrugged, continuing to watch the TV.
When he was finished, he got up and also took his bowl to the kitchen, and he coughed into his elbow as he placed his bowl in the sink. “Are you going to pay rent, at least?”
“Nope.” House popped the P and typed away on Wilson’s laptop, not bothering to look at the man. Wilson deadpanned at House until he decided to walk away and go back to his room, flopping onto his bed and falling asleep there.
The other man was searching for drug cocktails that he could inject his friend with to get him better, and he grinned devilishly when he found one that he had access to all of the drugs.
He leaned over slightly to see if Wilson’s door was open or not, and stood up and quickly made way to his bag when he saw it was closed. He pulled out what should have been a med-kit, and took out the drugs in it. He chose what he needed, and made sure all of the right ingredients were put into a syringe.
He slowly limped to Wilson’s room, opting out of using his cane so that he didn’t cause too much noise and wake him up. House opened his door carefully, and his nerves eased when he heard the loudest snore he’s ever heard in his life.
He ticked his tongue and made his way to Wilson, pulling out a sanitisation packet from his pocket. He lifted the sleeping man’s shirt and carefully rubbed it onto his back, freezing when he stirred. Pulling out the other packet, he wiped down the needle slowly and injected Wilson with the cocktail quickly.
He froze again, expecting Wilson to wake up and yell at him, but he didn’t. He was still fast asleep, and still snoring. House smiled in success and tossed the syringe into the trashcan by Wilson’s bed, and covered it up with crinkled tissues. He then left the room and closed the door, and went back into the kitchen where the laptop was.
House re-skimmed over the article with the side effects and he stopped when he saw something slightly alarming.
“Patient may fall unconscious for any time ranging from 16 hours to 2 days. Watch closely and monitor all the time. Any illnesses that the patient may have when the cocktail is injected will dimishness.”
“Shit.”
=======
Wilson woke up after twenty-six hours with cotton mouth, a diaper on, and no idea where he was until he saw House sitting on a chair reading a magazine.
“House?” He grumbled, lifting himself up to look at his clock. It was late, 1:24 in the morning to be exact. He looked back at House, and the man stood up and slapped the back of his hand onto Wilson’s forehead and held it there.
“Feels fine.” The man said, and he grabbed his cane and left the confused Wilson to his own devices.
Wilson didn’t know what happened, or what to do, so he chose to take a shower and freshen up. When he was done, he saw a glass of water on his bedside table and downed it immediately.
He sighed and stood there, unsure of what to do once again. That was until he noticed he felt much better than when he fell asleep.
He went to find House, and saw him in the kitchen again making what he assumed was an omelet. Staring into the back of House’s head, he felt that something was wrong.
He went to sleep with RSV and the worst headache and cough of his life, and now he felt like he could run a marathon.
“What did you do?” He questioned, and locked eyes with House when he turned around.
“What, no ‘thank you?’ No, ‘Oh my goodness, House. I feel so much better, thank you for your help and kindness?’” House mocked, tossing the omelet onto a plate and holding it out for Wilson.
Wilson felt iffy taking the food, but he still did and he sat down at the table as House served him a glass of orange juice.
“It’s two in the morning-” “I don’t care, eat your food.”
“M’kay.” Wilson didn’t argue and he grabbed his fork and ate, huffing down all of it and drinking every drop in the glass. “So, what’d you do?”
“I drugged you with seven different drugs.” House told him, grabbing Wilson’s plate and putting it in the sink before filling his glass back up with more juice. Wilson sat there and stared at him in disbelief, no words could come out of his mouth.
“Right.” Was the only word he could say, and he downed the drink in his glass. His mind was racing with many things he wanted to tell his friend.
He was in awe that he would put him so close to death, and that he would even think of doing such a thing that could one again, put him so close to death. It was insane of him to do, and he was flabbergasted. But what came out instead of yelling was,
“You cared that much?” House turned on the water to the sink and grabbed a sponge and soap and started doing the dishes, ignoring Wilson’s question.
That was the only answer Wilson needed, though, and he smiled at the back of House’s head.
“I’m telling your team when I go into work.”
“No the hell you aren’t!”
“Oh, yes the hell I am!”

Metastatic embolus from breast adenocarcinoma in the lungs
cancer cells are usually very metamorphic, which you can tell by the different shapes of the nuclei in this embolus. i love how you can see the metastasis inside a vessel perfectly in this picture!
Life saving knowledge !!
How to spot signs and symptoms of Breast Cancer
Brain Tumor

Introduction
Brain tumors represent a complex and diverse group of neoplasms that arise from abnormal growth of cells within the brain or its surrounding structures. These tumors can vary widely in terms of their location, size, aggressiveness, and clinical presentation. Understanding the intricacies of brain tumors, including their diagnosis, treatment, and prognosis, requires a comprehensive approach that integrates medical expertise, advanced imaging modalities, and personalized therapeutic interventions.
Diagnosis of Brain Tumor

The diagnosis of a brain tumor typically begins with a thorough clinical evaluation, including a detailed medical history and neurological examination. Symptoms suggestive of a brain tumor may include persistent headaches, seizures, cognitive deficits, changes in behavior or personality, and focal neurological deficits such as weakness or sensory disturbances. However, it’s essential to recognize that many of these symptoms are nonspecific and can be caused by various other conditions.
To confirm the presence of a brain tumor and characterize its specific features, a variety of imaging studies and laboratory tests may be employed. These include computed tomography (CT) scans, magnetic resonance imaging (MRI), and positron emission tomography (PET) scans. CT scans provide detailed cross-sectional images of the brain and are often the initial imaging modality used to assess patients with suspected brain tumors due to their widespread availability and rapid results. MRI, on the other hand, offers superior soft tissue contrast and is particularly useful for delineating the precise location and extent of brain tumors. In some cases, contrast-enhanced MRI with gadolinium-based contrast agents may be performed to enhance visualization of tumor tissue and surrounding structures.
Advanced MRI techniques, such as functional MRI (fMRI), magnetic resonance spectroscopy (MRS), and perfusion-weighted imaging (PWI), can provide additional information about the functional characteristics and metabolic activity of brain tumors. These modalities play a crucial role in treatment planning and assessing tumor response to therapy.
In select cases, a PET scan may be utilized to evaluate the metabolic activity of brain tumors and differentiate between benign and malignant lesions. PET imaging with radiopharmaceutical tracers such as fluorodeoxyglucose (FDG) can help identify areas of increased glucose metabolism, which are typically indicative of rapidly growing tumor cells. Additionally, molecular imaging techniques targeting specific biomarkers may offer insights into the molecular profile and biological behavior of brain tumors, facilitating personalized treatment strategies.
Tissue Sampling and Histopathological Evaluation: While imaging studies provide valuable information about the radiographic characteristics of brain tumors, definitive diagnosis often requires histopathological analysis of tissue samples obtained via biopsy or surgical resection. Tissue sampling allows for detailed microscopic examination of tumor cells, assessment of histological features, and determination of tumor grade, which plays a crucial role in prognostication and treatment planning.
Brain tumor grading is based on the World Health Organization (WHO) classification system, which stratifies tumors into different grades (I-IV) based on their histological features and biological behavior. Grade I tumors are typically slow-growing and well-differentiated, while grade IV tumors are highly aggressive and rapidly proliferating. Intermediate grades (II-III) exhibit varying degrees of aggressiveness and cellular atypia.
Prognostic Factors and Treatment Consideration

The prognosis of patients with brain tumors is influenced by various factors, including tumor type, grade, location, extent of resection, molecular characteristics, and patient-specific factors such as age and overall health status. High-grade tumors, such as glioblastoma multiforme, are associated with poorer outcomes compared to low-grade tumors, necessitating more aggressive treatment approaches.
Treatment strategies for brain tumors are highly individualized and may encompass a combination of surgical resection, radiation therapy, chemotherapy, targeted therapy, and supportive care measures. The goals of treatment are to achieve maximal tumor control while preserving neurological function and quality of life. Surgical resection is often the initial step in the management of operable brain tumors, with the aim of achieving gross total resection whenever feasible. However, the proximity of tumors to critical brain structures and eloquent areas may limit the extent of surgical resection and necessitate adjuvant therapies.
Surgical Management of Brain Tumor

Surgical approaches to brain tumor resection have evolved significantly with advances in neuroimaging, neurosurgical techniques, and intraoperative navigation systems. Traditional open craniotomy remains the standard approach for many brain tumors, allowing for direct access to the intracranial lesion. Microsurgical techniques, including the use of operating microscopes and intraoperative neuro navigation systems, enable precise tumor localization and maximal safe resection while minimizing damage to adjacent healthy brain tissue.
In recent years, minimally invasive approaches such as endoscopic endonasal surgery and keyhole craniotomy have gained popularity for select brain tumors, offering advantages such as smaller incisions, reduced surgical morbidity, and faster recovery times. Endoscopic techniques, in particular, allow for access to deep-seated lesions through natural orifices, such as the nasal cavity, thereby avoiding the need for extensive craniotomies and brain retraction.
Radiation Therapy for Brain Tumors

Radiation therapy plays a critical role in the management of both primary and metastatic brain tumors, offering precise and localized delivery of ionizing radiation to target tumor cells while sparing adjacent normal brain tissue. External beam radiation therapy (EBRT) is the most commonly utilized modality, utilizing high-energy X-rays or protons to deliver radiation to the tumor site over multiple treatment sessions. Techniques such as intensity-modulated radiation therapy (IMRT) and stereotactic radiosurgery (SRS) allow for highly conformal dose delivery, enabling escalation of radiation doses to the tumor while minimizing toxicity to surrounding critical structures.
In addition to conventional EBRT, brachytherapy techniques may be employed for selected cases, involving the placement of radioactive sources directly into or adjacent to the tumor cavity during surgical resection. This allows for localized delivery of high-dose radiation while minimizing exposure to healthy tissues. Proton therapy, a form of particle therapy, offers the advantage of improved dose conformity and reduced integral dose to surrounding tissues compared to conventional photon-based radiation therapy. Proton therapy is particularly beneficial for treating pediatric brain tumors and tumors located near critical structures, such as the optic nerves and brainstem.
Chemotherapy and Targeted Therapy: Chemotherapy plays a crucial role in the management of certain brain tumors, particularly high-grade gliomas and metastatic lesions. Chemotherapeutic agents may be administered orally, intravenously, or intracranially, either as monotherapy or in combination with other treatment modalities. The choice of chemotherapy regimen depends on factors such as tumor type, molecular characteristics, and patient-specific considerations.
Targeted therapy has emerged as a promising treatment approach for select brain tumors, leveraging the identification of specific molecular targets or pathways implicated in tumor growth and progression. Targeted agents may include small molecule inhibitors, monoclonal antibodies, or immunotherapeutic agents designed to selectively target tumor cells while sparing normal tissues. Biomarker-driven approaches, such as molecular profiling and genetic testing, help identify patients who are most likely to benefit from targeted therapies, enabling a personalized approach to treatment selection.
Recovery and Rehabilitation

Recovery following treatment for brain tumors often requires comprehensive rehabilitation efforts aimed at optimizing functional outcomes and quality of life. Physical therapy, occupational therapy, speech therapy, and cognitive rehabilitation play important roles in addressing deficits related to motor function, activities of daily living, communication, and cognition. Additionally, psychosocial support services and caregiver education are essential components of the multidisciplinary care team, providing emotional support and practical assistance to patients and their families throughout the treatment and recovery process.
Conclusion
In conclusion, the management of brain tumors necessitates a multidisciplinary and individualized approach that integrates advances in diagnostic imaging, surgical techniques, radiation therapy, chemotherapy, targeted therapy, and supportive care interventions. Collaborative decision-making between patients, healthcare providers, and allied health professionals is paramount in optimizing treatment outcomes and enhancing quality of life for individuals affected by brain tumors. Ongoing research efforts aimed at elucidating the molecular mechanisms underlying tumorigenesis, identifying novel therapeutic targets, and refining treatment strategies offer hope for continued advancements in the field of neuro-oncology and improved outcomes for patients with brain tumors.
We wish you all the best in your medical education journey. In case you need any guidance or assistance during the learning process, do not hesitate to reach out to us.
Email at;
williamsassignmenthelpfredrick@gmail.com